Database Open Access
Pressure, flow, and dynamic thoraco-abdominal circumferences data for adults breathing under CPAP therapy
Ella Frances Sophia Guy , Jennifer Knopp , Theodore Lerios , James Geoffrey Chase
Published: Jan. 25, 2023. Version: 1.0.0
When using this resource, please cite:
(show more options)
Guy, E. F. S., Knopp, J., Lerios, T., & Chase, J. G. (2023). Pressure, flow, and dynamic thoraco-abdominal circumferences data for adults breathing under CPAP therapy (version 1.0.0). PhysioNet. https://doi.org/10.13026/25q9-y416.
Please include the standard citation for PhysioNet:
(show more options)
Goldberger, A., Amaral, L., Glass, L., Hausdorff, J., Ivanov, P. C., Mark, R., ... & Stanley, H. E. (2000). PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation [Online]. 101 (23), pp. e215–e220.
Abstract
A respiratory pressure, flow, and dynamic circumference (chest and abdominal) dataset was collected from 30 healthy adults at the University of Canterbury under Human Research Ethics Committee (HREC) ethics. Pressure and flow data was collected using a bi-directional Venturi, with data combined in post-collection processing. Dynamic circumferences were measured using inelastic band tape measures attached to rotary encoders capturing expansion and contraction. Data was collected at zero end-expiratory pressure (ZEEP) and with continuous positive airway pressure (CPAP) ventilation, at positive end-expiratory pressure (PEEP) settings of 4 and 8 cmH2O. Data was also collected over three breath types, in which subjects were instructed to breathe normally, to pant as fast as possible, and to breathe as deeply as possible. Recording times were set to 65 seconds for normal and deep breathing, and 35 seconds for panting trials. Subjects self-determined rest time between trials. A questionnaire was used to collect relevant demographic data (sex, height, age, weight, and history of smoking or asthma). The dataset was collected to inform and validate model-based respiratory monitoring systems, with the ultimate goal of shifting respiratory testing from specialist clinical settings to primary care and home settings
Background
Respiratory diseases are of increasing burden to modern society [1, 2]. Currently, the diagnosis and treatment of respiratory disease are reliant on specialist clinical testing which is conducted in specialist clinical settings [3]. Increasing the capabilities of at-home respiratory disease monitoring, would de-burden the healthcare system and increase treatment capacity. For at-home testing to be feasibly implemented, remote model-based methods of respiratory assessment must match or exceed current clinical examination/observation methods. Respiratory datasets are critical in informing and validating these models.
In respiration, inspiration is driven by the expansion of the thorax, which creates a negative pressure gradient and generates a flow of air into the lungs [4, 5]. The primary muscle of respiration is the diaphragm which distends downward towards the abdomen to increase lung volume [4, 5]. Lung volume is also increased by external intercostal contraction, which raises the ribcage [4, 5]. Expiration is predominantly passive in normal breathing, and driven by elastic recoil of lung tissue, however, can be actively driven by eccentric activation of the diaphragm [4, 5].
Respiratory disease can be characterised by the combination of physiological obstructive or restrictive abnormalities developed [3, 6]. Obstructive abnormalities are those which occlude airways (constriction, inflammation, and collapse) and cause increased airway resistance [3, 7, 8]. Restrictive abnormalities are those which stiffen lung tissue (by scaring/fibrosis) or the thorax (in cases of severe burns and obesity) [3, 9-12]. Clinically, changes in respiratory state and potential abnormalities are primarily assessed by observed changes to breath patterns, palpation, percussion, auscultation and oximetry [3, 13-15].
Mechanical ventilation (MV) is a primary tool in the treatment of respiratory disease [16]. MV is split into invasive (IMV) or non-invasive (NIMV) methods. Where, in IMV, patients are sedated and intubated with all work of breathing (WOB) done by the ventilator [16-18]. Conversely, in NIMV, patients breathe spontaneously with support from the ventilator. NIMV support is commonly provided by positive airway pressure (PAP) at a set positive end-expiratory pressure (PEEP). PEEP is set at either a single continuous level (CPAP), bilevel (BiPAP), or automatically adjust within a range (APAP). PAP is commonly used in home settings, particularly overnight in the treatment of sleep-disordered breathing, including obstructive sleep apnea (OSA) [19].
Model-based methods of assessing respiratory function require the ability to identify respiratory abnormalities, signs of distress, and response to NIMV, for implementation in an at-home monitoring system. Model-based methods have successfully identified patient effort, lung elastance, and airway resistance, with and without MV support [20-29]. However, elucidation of the contributions of respiratory muscles would provide a more comprehensive assessment of patient effort and fatigue in respiration, as well as provide validation of existing models. Hence, the dataset presented was collected to validate and improve models of the respiratory system. With the ultimate goal of shifting respiratory testing from clinical settings to home and primary care settings. Thus, improving access to care and the clarity of information provided to patients.
In order to assess muscular contributions, dynamic circumference tapes were developed [30]. In collecting this preliminary dataset, these tapes were placed around the chest (armpit level with the tape sitting on the flat upper portion of the sternum), and the abdomen (narrowest section/waist). The tapes provided a fast, low-cost, and simple assessment of thoraco-abdominal distribution of lung volume, indicative of muscular recruitment. Designs for these devices are published open-access [30].
Methods
Data was collected using a custom bi-directional venturi device with dynamic thoracic and abdominal circumferential monitoring [30]. The subjects breathed through a CPAP mask (FreeMotion RT041, Fisher and Paykel Healthcare, New Zealand) connected to a HEPA filter (HMEF 002874, Smiths Medical, Minneapolis, MN, USA) during the trial. The custom device was connected in series with this breathing circuit between the filter and the CPAP circuitry. Circumferential monitoring bands were placed around the thorax and abdomen of the subject at armpit and waist height respectively. A Matlab (Matlab 2020a, The Mathworks Inc, Natick, MA, USA) script was used to sample data (at 100Hz) for each section of the trial (Breath Rate and PEEP Setting Combinations)
The trial protocol involved the subject breathing at 3 rates: normal/passive breathing for 60 seconds (subjects instructed to breathe normally); panting for 30 seconds (subjects instructed to pant as fast as possible); then deep breathing for 60 seconds (subjects instructed to breathe as deeply as possible). These three breath rates were repeated at PEEP settings of 0 (ZEEP), 4, and 8 cmH2O. Between each of these 9 breathing tests were periods of rest and the subject self-indicated when they were recovered and ready for subsequent tests. Ethical consent for the trial was granted by the Human Ethics Committee at the University of Canterbury (Ref: HEC 2020/14/LR) with amendments accepted 22 November 2021.
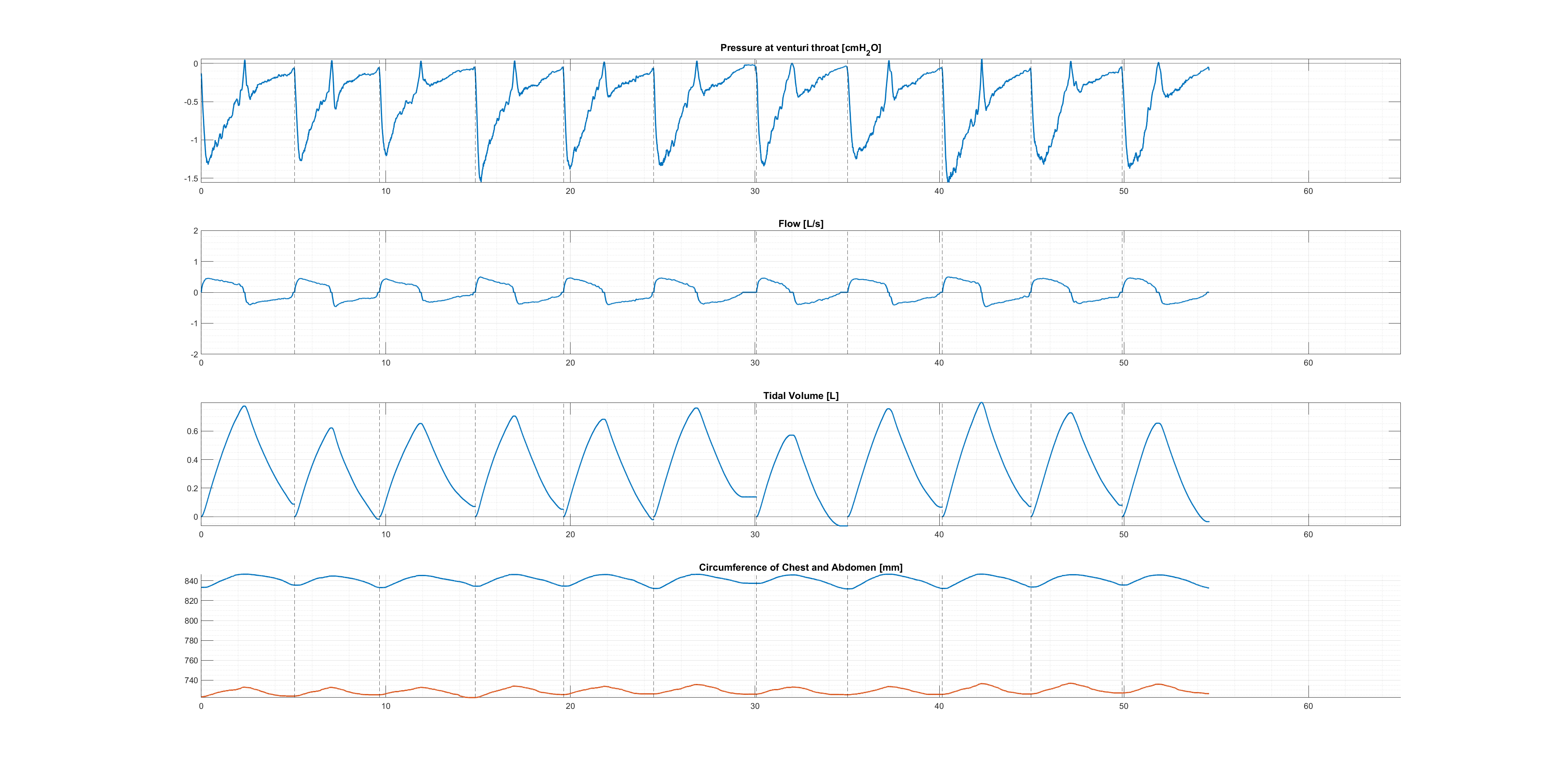
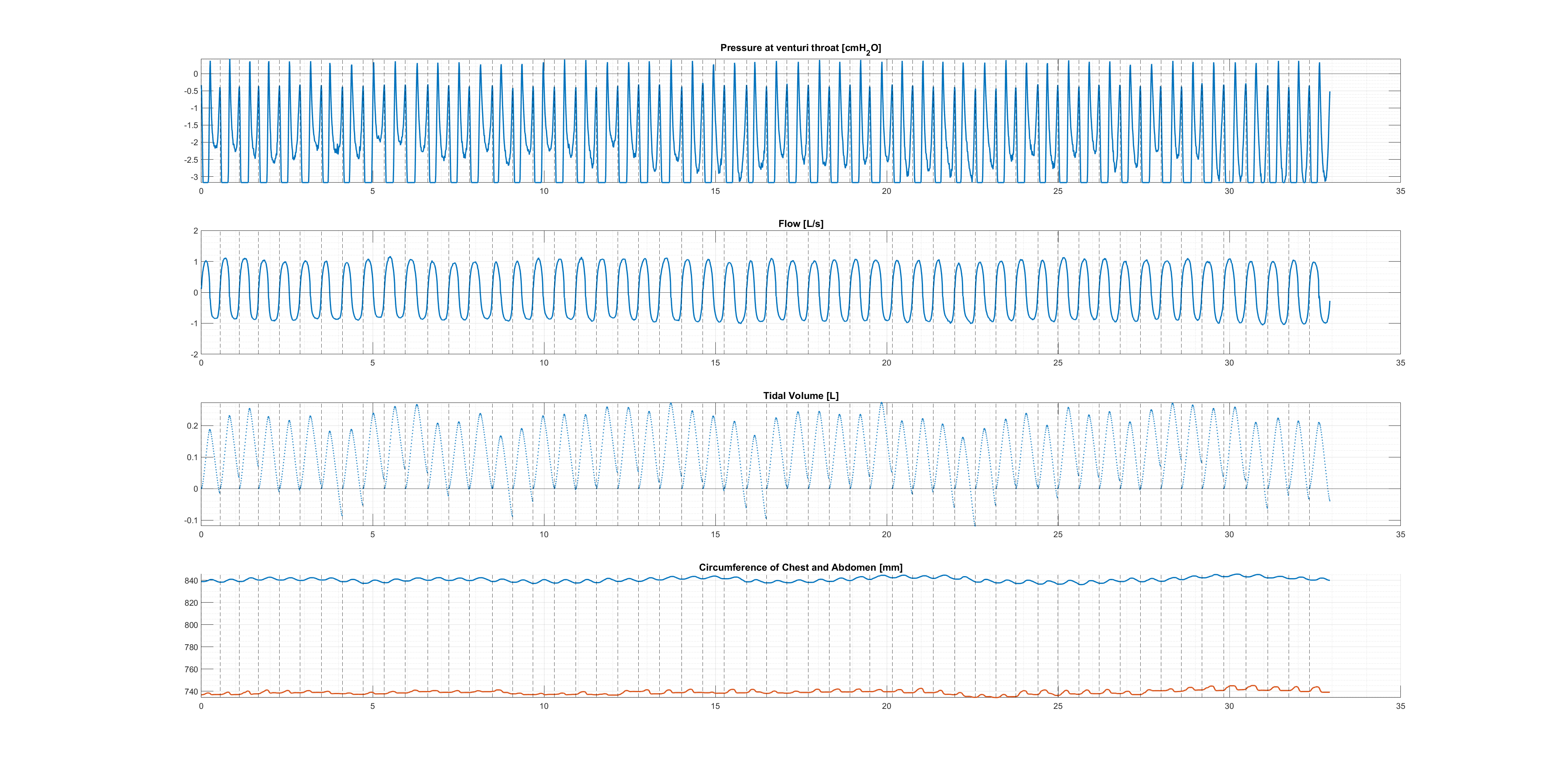
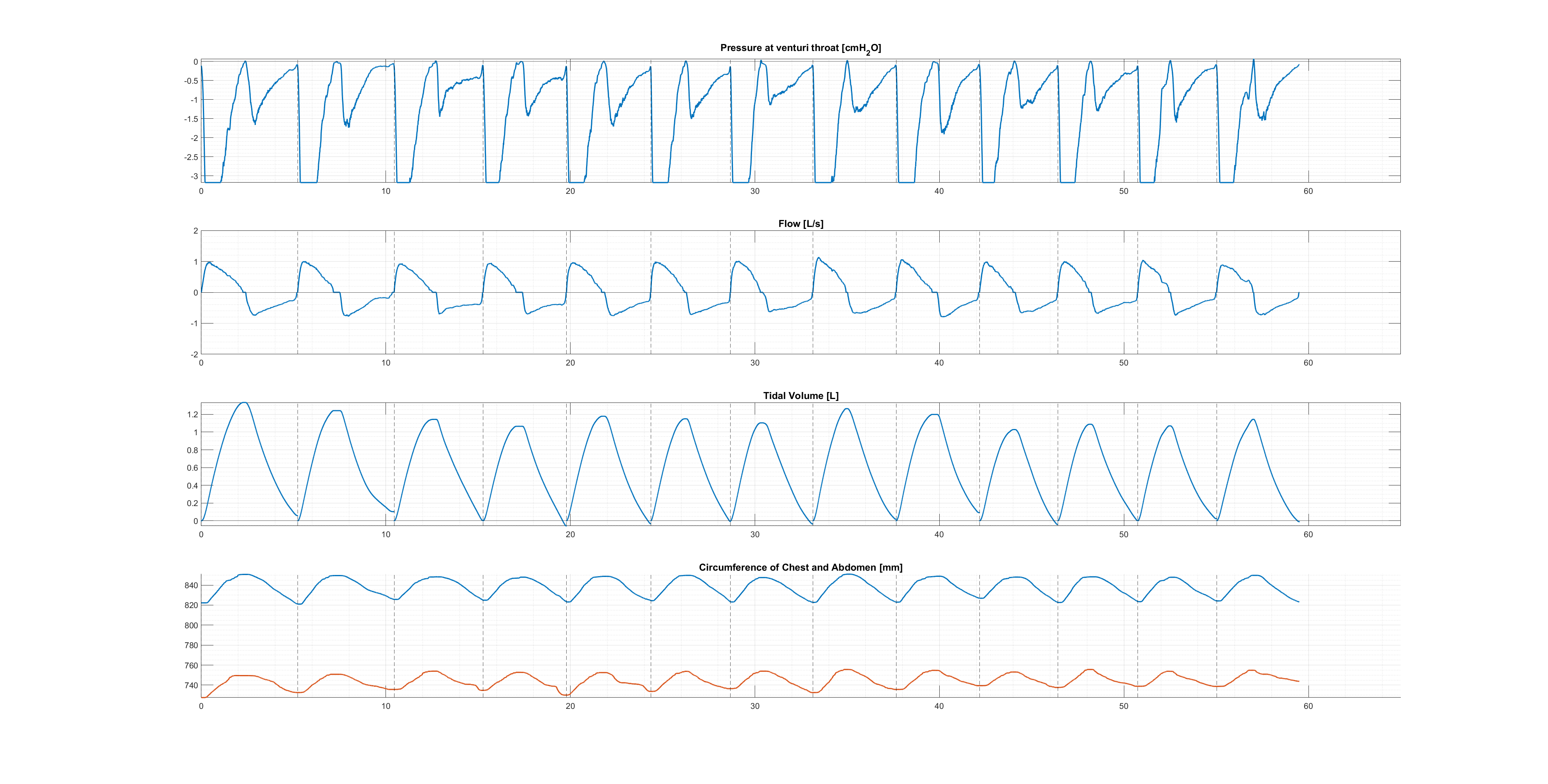
A Matlab data processing script was used to identify breaths, combine inspiratory and expiratory data into comprehensive breath sets and compute tidal volumes. Example plots of data are included below (Figures 1-3) for Subject 3 at ZEEP (normal, panting, and deep breathing respectively).
Data Description
Data was collected from 30 healthy subjects, aged 19-37, recruited via advertisement at the University of Canterbury, under ethical approval and full informed consent. The trial included an even split of sex (15 male and 15 female), smokers, vapers and asthmatics. Subject data was de-identified using subject numbers unassociated to signed consent forms. Demographic data was collected for each subject number (sex, height, weight, age, smoking history, history of asthma, and whether any of the trials made it feel harder or easier to breathe). Demographic data is included in a spreadsheet by subject. A ‘README.txt’ file is included to describe the location, naming, and contents of files in this dataset.
Raw datasets are saved as csv files against time [s], with raw measurements of: gauge pressure at venturi throat; inspiratory differential pressure; expiratory differential pressure; chest circumference rotary encoder counts; abdominal circumference rotary encoder counts. Files are saved in 'raw-data' under folders by subject number ('01' through to '30'). Files are saved in these folders by PEEP setting and breath rate type (Subject Number is also referenced) both processed into relevant units (e.g. 'CPAP2022_Subject1_0cmH2O_deep.csv') and as raw ADC outputs (e.g. 'CPAP2022_Subject1_0cmH2O_deep_raw.csv').
Processed datasets are saved as csv files containing: time [s]; pressure [cmH2O]; flow [L/s]; tidal volume [L]; inspiratory start point indices; chest circumference [mm]; and abdominal circumference [mm]. Files are saved in 'processed-data' under folders by PEEP setting (0, 4, or 8) and breath rate type (norm, pant, or deep) e.g. '0cmH2O_deep'. Hence, each folder contains a data file for each Subject Number (PEEP and breath type is also referenced) e.g. 'CPAP2022_ProcessedData_Subject1_0cmH2O_deep.csv'.
Demographic data are attached as 'subject-info.csv', which contains the relevant self-reported medical information for the 30 subjects. Columns A to M respectively contain: Subject Number, Sex (M/F), Height(cm), Weight (kg), Age (years), Smoker and/or Vaper (Yes/No), Smoking Frequency (units included in column values), Duration of smoking (units included in column value), Asthmatic (Yes/No), Medication name, Frequency of use of asthma medication (units included in column value), any trials the subject perceived to make it harder to breathe (PEEP setting [cmH2O]), and any trials the subject perceived to make it easier to breathe (PEEP setting [cmH2O]).
Example plots of data are included (Figures 1-3>) for Subject 3 at ZEEP (normal, panting, and deep breathing respectively) are included alongside the MATLAB data collection code used to generate them ('FigureGenerationCode.m' in ‘code’ folder).
Usage Notes
The dataset can be used in the development and application of pulmonary mechanics models. Pressure, flow and volume can be used as inputs to pulmonary mechanics models to assess their fit and accuracy in identifying patient-specific parameters (e.g. lung elastance and airway resistance). Additionally, the auxiliary dynamic circumferential monitoring allows for the secondary validation of these models as this data provides two separate methods of estimating changes in lung volume and muscular recruitment. The trial cohort includes an even split of male and females to assess and sex-based differences in pulmonary mechanics. Asthmatics and smokers were also included in the trial for preliminary assessment of any pathophysiological implications to pulmonary mechanics and model-based assessment of these subjects.
The trial was conducted under HREC ethical consent at the University of Canterbury (HEC 2020/14/LR). The trial was conducted using reproducible hardware and code that has been made openly available [30], and so can be augmented and tailored to adjacent future research applications. An example MATLAB script which plots the data (Figures 1-3), has been included in this repository as 'FigureGenerationCode.m', other data collection code and files can be found in a HardwareX publication [30].
Ethics
Ethical consent for the trial by the Human Ethics Committee at the University of Canterbury (Ref: HEC 2020/14/LR), with ammendments accepted on 22 NOVEMBER 2021.
Acknowledgements
This work was funded by a grant from the New Zealand Government through the Ministry of Business, Innovation, and Employment.
Conflicts of Interest
The authors have no conflcits of interest to declare.
References
- P. Burney, D. Jarvis, R. J. T. I. J. o. T. Perez-Padilla, and L. Disease, "The global burden of chronic respiratory disease in adults," The International Journal of Tuberculosis and Lung Disease, vol. 19, no. 1, pp. 10-20, 2015.
- L. Dwyer-Lindgren et al., "Trends and patterns of differences in chronic respiratory disease mortality among US counties, 1980-2014," vol. 318, no. 12, pp. 1136-1149, 2017.
- T. Des Jardins and G. G. Burton, Clinical Manifestations & Assessment of Respiratory Disease E-Book. Elsevier Health Sciences, 2019.
- J. B. West and A. M. Luks, West's Respiratory Physiology. Lippincott Williams & Wilkins, 2020.
- G. J. Tortora and B. H. Derrickson, Principles of anatomy and physiology. John Wiley & Sons, 2018.
- R. Pellegrino et al., "Interpretative strategies for lung function tests," European Respiratory Journal, vol. 26, no. 5, p. 948, 2005.
- N. R. MacIntyre, "Muscle dysfunction associated with chronic obstructive pulmonary disease," Respiratory care, vol. 51, no. 8, pp. 840-852, 2006.
- J. Butler, C. G. Caro, R. Alcala, and A. B. J. T. J. o. c. i. DuBois, "Physiological factors affecting airway resistance in normal subjects and in patients with obstructive respiratory disease," vol. 39, no. 4, pp. 584-591, 1960.
- L. C. Melo, M. A. M. d. Silva, and A. C. d. N. Calles, "Obesity and lung function: a systematic review," Einstein (Sao Paulo), vol. 12, pp. 120-125, 2014.
- V. S. Taskar and D. B. Coultas, "Is idiopathic pulmonary fibrosis an environmental disease?," Proceedings of the American Thoracic Society, vol. 3, no. 4, pp. 293-298, 2006.
- D. Sulli, A. Dhopte, and K. Agrawal, "Impact of burn contractures of chest wall and their surgical release on pulmonary function," Burns, vol. 45, no. 4, pp. 929-935, 2019.
- P. J. Martinez-Pitre, B. R. Sabbula, and M. Cascella, "Restrictive lung disease," 2020.
- T. Flenady, T. Dwyer, and J. Applegarth, "Accurate respiratory rates count: So should you!," Australasian emergency nursing journal, vol. 20, no. 1, pp. 45-47, 2017.
- G. Cacho, J. L. Pérez-Calle, A. Barbado, J. L. Lledó, R. Ojea, and C. M. Fernández-Rodríguez, "Capnography is superior to pulse oximetry for the detection of respiratory depression during colonoscopy," Revista espanola de enfermedades digestivas, vol. 102, no. 2, p. 86, 2010.
- J. J. Pretto, T. Roebuck, L. Beckert, and G. Hamilton, "Clinical use of pulse oximetry: official guidelines from the T horacic S ociety of A ustralia and N ew Z ealand," Respirology, vol. 19, no. 1, pp. 38-46, 2014.
- S. S. Carson, C. E. Cox, G. M. Holmes, A. Howard, and T. S. Carey, "The changing epidemiology of mechanical ventilation: a population-based study," Journal of intensive care medicine, vol. 21, no. 3, pp. 173-182, 2006.
- B. Popat and A. T. Jones, "Invasive and non-invasive mechanical ventilation," Medicine, vol. 40, no. 6, pp. 298-304, 2012/06/01/ 2012.
- C. Carter, M. Osborn, G. Agagah, H. Aedy, and J. Notter, "COVID-19 disease: invasive ventilation," (in eng), Clinics in Integrated Care, vol. 1, pp. 100004-100004, 2020.
- N. Stasche, "Selective indication for positive airway pressure (PAP) in sleep-related breathing disorders with obstruction," GMS Current Topics in Otorhinolaryngology, Head and Neck Surgery, vol. 5, 2006.
- J. H. T. Bates, Lung mechanics: an inverse modeling approach (no. Book, Whole). Cambridge, UK;New York;: Cambridge University Press, 2009.
- Y. S. Chiew, J. G. Chase, G. M. Shaw, A. Sundaresan, and T. Desaive, "Model-based PEEP optimisation in mechanical ventilation," BioMedical Engineering OnLine, vol. 10, no. 1, p. 111, 2011/12/23 2011.
- Y. S. Chiew et al., "Time-varying respiratory system elastance: a physiological model for patients who are spontaneously breathing," (in eng), PloS one, vol. 10, no. 1, pp. e0114847-e0114847, 2015.
- S. E. Morton et al., "Optimising mechanical ventilation through model-based methods and automation," Annual Reviews in Control, vol. 48, pp. 369-382, 2019/01/01/ 2019.
- J. G. Chase et al., "Next-generation, personalised, model-based critical care medicine: a state-of-the art review of in silico virtual patient models, methods, and cohorts, and how to validation them," BioMedical Engineering OnLine, vol. 17, no. 1, p. 24, 2018/02/20 2018.
- S. E. Rees, "The Intelligent Ventilator (INVENT) project: the role of mathematical models in translating physiological knowledge into clinical practice," (in eng), Comput Methods Programs Biomed, vol. 104 Suppl 1, pp. S1-29, Dec 2011.
- S. E. Rees et al., "Using physiological models and decision theory for selecting appropriate ventilator settings," vol. 20, no. 6, pp. 421-429, 2006.
- J. L. Knopp, E. Guy, K. T. Kim, G. M. Shaw, and J. G. Chase, "B-spline modelling of inspiratory drive in NAVA-ventilated patients," IFAC-PapersOnLine, vol. 54, no. 15, pp. 103-108, 2021/01/01/ 2021.
- E. F. S. Guy, J. L. Knopp, and J. G. Chase, "Pilot study of model-based estimation of inspiratory driving pressure in CPAP ventilation," IFAC-PapersOnLine, vol. 54, no. 15, pp. 109-114, 2021/01/01/ 2021.
- E. F. S. Guy, J. G. Chase, J. L. Knopp, and G. M. Shaw, "Quantifying ventilator unloading in CPAP ventilation," Computers in Biology and Medicine, vol. 142, p. 105225, 2022/03/01/ 2022.
- E. F. S. Guy, J. Geoffrey Chase, and L. R. Holder-Pearson, "Respiratory bi-directional pressure and flow data collection device with thoracic and abdominal circumferential monitoring," HardwareX, vol. 12, p. e00354, 2022/10/01/ 2022.
Access
Access Policy:
Anyone can access the files, as long as they conform to the terms of the specified license.
License (for files):
Creative Commons Attribution 4.0 International Public License
Discovery
DOI (version 1.0.0):
https://doi.org/10.13026/25q9-y416
DOI (latest version):
https://doi.org/10.13026/wmzm-d487
Corresponding Author
Files
Total uncompressed size: 304.5 MB.
Access the files
- Download the ZIP file (79.9 MB)
-
Download the files using your terminal:
wget -r -N -c -np https://physionet.org/files/pressure-flow-circum-cpap/1.0.0/
-
Download the files using AWS command line tools:
aws s3 sync s3://physionet-open/pressure-flow-circum-cpap/1.0.0/ DESTINATION
| Name | Size | Modified |
|---|---|---|
| code | ||
| processed-data | ||
| raw-data | ||
| Figure1.png (download) | 281.5 KB | 2022-12-20 |
| Figure2.png (download) | 423.3 KB | 2022-12-20 |
| Figure3.png (download) | 341.3 KB | 2022-12-20 |
| LICENSE.txt (download) | 14.5 KB | 2023-01-24 |
| README.txt (download) | 3.3 KB | 2023-01-11 |
| SHA256SUMS.txt (download) | 94.2 KB | 2023-01-25 |
| subject-info.csv (download) | 12.7 KB | 2022-07-21 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}