Database Open Access
CPAP Pressure and Flow Data from a Local Trial of 30 Adults at the University of Canterbury
Ella Guy , Jennifer Knopp , Geoff Chase
Published: March 24, 2022. Version: 1.0.1
When using this resource, please cite:
(show more options)
Guy, E., Knopp, J., & Chase, G. (2022). CPAP Pressure and Flow Data from a Local Trial of 30 Adults at the University of Canterbury (version 1.0.1). PhysioNet. https://doi.org/10.13026/xfae-vv63.
Please include the standard citation for PhysioNet:
(show more options)
Goldberger, A., Amaral, L., Glass, L., Hausdorff, J., Ivanov, P. C., Mark, R., ... & Stanley, H. E. (2000). PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation [Online]. 101 (23), pp. e215–e220.
Abstract
A pressure and flow dataset for CPAP (continuous positive airway pressure) breathing obtained from 30 subjects for model-based identification of patient-specific lung mechanics using a specially designed sensor system comprising an array of differential pressure sensors (Sensirion AG SDP816-125PA) and gauge pressure sensors (NXP MPVZ4006GW7U). Relevant medical information was collected using a questionnaire, including: sex; age; weight; height; smoking history; and history of asthma. Subjects were tasked with breathing at five different rates (including passive) from very slow to very fast breathing, matched to an online pacing sound and video, at two different levels of CPAP (4 and 7 cmH2O) for between 50 and 180 seconds depending on rate. Each data set for a breathing rate comprises ~17 breaths, including rest periods between breathing rates and CPAP levels. Data with significant observed sensor error was removed during processing. A better-fitted mask would be expected to reduce error in fully capturing expiration by reducing leaks around the masks seal with the face. The sensors measure inspiration and expiration using separate unidirectional differential flow sensors, which are combined in post-processing to for complete breathing data.
Background
CPAP is a form of non-invasive ventilation used in both hospital and home settings to treat respiratory conditions and wean patients off invasive ventilation [1, 2]. Respiratory conditions are categorised by the presence or combination of obstructive or restrictive abnormalities [3]. Obstructive abnormalities result in airway restrictions reducing the rate of exhalation. The pressure provided in CPAP ventilation acts as a “pneumatic splint” to maintain open airways [4]. Restrictive abnormalities occur due to increased stiffness of the lung tissue due to fibrotic scarring, pressure on the lungs or lack of inspiratory muscle function. CPAP reduces the required pressure gradient from lung expansion (work of breathing (WOB)) to drive airflow to assist breathing. Reliable model-based methods of assessment of airway resistance (R) and lung elastance (E) would inform more patient-specific CPAP treatment [5].
An important CPAP setting is the positive end expiratory pressure (PEEP). In both hospital and outpatient scenarios, insufficient PEEP can result in under-oxygenation or airway collapse [6, 7]. Conversely, excessive PEEP can cause pulmonary barotrauma [6, 7]. Rupture of this tissue (emphysema) and air trapping can lead to pneumothorax [6, 7]. Finally, excessive PEEP can also cause increases in intracranial pressure due to intrathoracic pressure increases, as well as increased fluid retention [6, 8].
Protocols for setting PEEP vary significantly and are predominantly based on clinical judgment of the comparative foreseeable risks of hyperinflation and under oxygenation [4, 9, 10]. This approach results in highly variable care, as well as potential inequity and issues of unconscious bias [11]. In CPAP ventilation, the “CPAP Titration Protocol” [4, 12, 13] is commonly used to titrate PEEP based on patient blood oxygenation or symptoms of airway collapse. However, lung response is driven by lung mechanics, specifically E and R, where a recent study of Acute Respiratory Distress Syndrome (ARDS) patients showed optimising ventilation pressures based on lung elastance, rather than tidal volume or peak pressures, could be more beneficial to patient outcomes [14]. Thus, there is potential to optimise PEEP in CPAP if reliable, non-invasive, real-time measures of lung mechanics, including elastance, can be assessed at the bedside.
One such measure of lung elastance can be obtained using model-based methods at the bedside. These methods use relatively simple, readily identifiable compartment models [15-21], which describe lung behaviour as a function of respiratory elastance (E) and airway resistance (R). Such models have been effective in fully sedated patients [16, 18], where the work of breathing (WOB) is done by the ventilator and passive respiratory mechanics (E and R) can be identified from airway pressure and flow profiles. They have not yet been successfully adapted to spontaneous breathing modes, which are common in invasive MV and comprise all non-invasive MV types, as spontaneous breathing masks identification of these respiratory parameters [17, 22-24], complicating model-based analyses and protocols.
This project collected a unique dataset of airway flow/pressure from healthy subjects on Continuous Positive Airway Pressure (CPAP) ventilation, for model-based analyses of patient lung mechanics (including E and R) and work of breathing in spontaneously breathing subjects. The data set is useful for model-based analyses, as well as clinically relevant in providing ‘real-world’ data for analysis and/or training not available in the limited, often smoothed and idealised literature data. The overall project aim is to develop protocols for optimising MV settings in spontaneous breathing patients and ventilation modes without having to rely on physiological responses to insufficient or excessive PEEP settings.
Methods
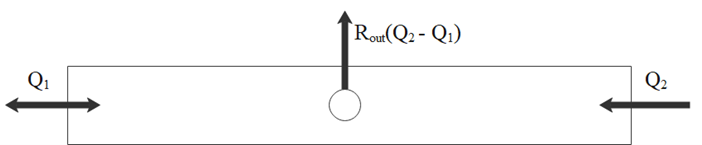
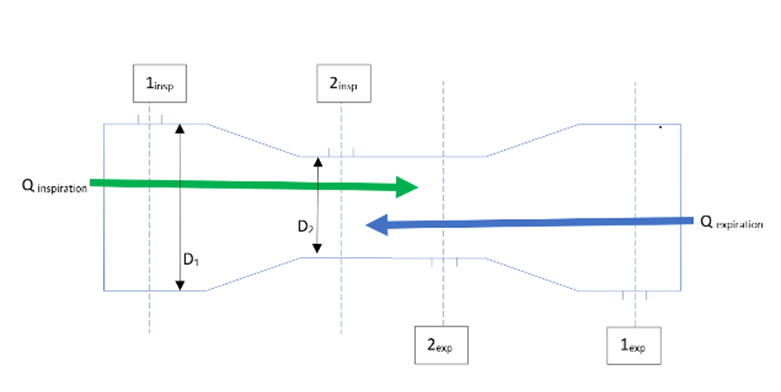
Data was collected using a customised sensor system consisting of two mutiVenturi tubes on either side of the CPAP expiration hole (Figure 1). The dual-Venturi apparatus (Figure 2) with central expiration hole was 3D printed to fit standard CPAP masks (FreeMotion RT041, Fisher and Paykel Healthcare, New Zealand), with an inner diameter of 15mm (D1) and a Venturi diameter of 12mm (D2). The data set thus captures flow delivered from the CPAP machine and flow delivered to the CPAP mask.
Differential pressure sensors connected in both directions over the Venturi restrictions enable flow measurement (Figure 3). Static pressure was also measured at both locations. As flow sensors were uni-directional, both inspiratory and expiratory flow were measured at each Venturi tube separately, using two sets of differential pressure (flow) sensors with data combined in post-processing. Data was recorded at a frequency of 83.33 Hz, and then resampled to 100 Hz for ease of use, from of the sensors via a central Arduino unit (Nano V3, Baite Electronics, China) in analogue-to-digital converter (ADC) counts, which was serially interfaced with a laptop for data acquisition. Sensors were calibrated against a known flow profile obtained from a hospital-grade mechanical ventilator (PB840, Puritan Bennet, USA, using CURESoft [25]).
The trial protocol consisted of a sequence of breaths at different breathing rates repeated at nominal PEEP levels of 4 and 7 cmH20. Breathing rates included short (60 breaths per min), medium-short (30 breaths per min), medium-long (9 breaths per min), and long (6 breaths per min). At each breathing rate, 17 breaths were cued for inhalation and exhalation by an audio-visual pacer. Data recording also captured baseline breathing at rest before the trial ("Normal" breathing), with rest intervals of 30-90 seconds also occurring after each cued breath sequence at the specified rate, as determined by subjects.
Raw data was processed in Matlab (Matlab 2020a, The Mathworks Inc, Natick, MA, USA), with pressure values calculated based on data sheet information for each of the sensors [26, 27]. Flow was calculated from differential pressure across each Venturi as a function of its relationship to the diameter change at the restriction via Bernoulli’s equation and conservation of mass. Inspiratory and expiratory flow were merged into a single multidirectional flow dataset for each Venturi by a minimum inspiration length and volume based on the cued breath rate. The final data set thus has flow in [L/s] and pressure in [cmH2O] at the entry to the CPAP mask (upstream of the expiration hole) and downstream of the expiration hole
Data Description
Data was collected from 30 healthy subjects recruited via advertisement at the University of Canterbury, under ethical approval and full informed consent. The study population comprised an even split of male and female participants ranging from 19 – 58 years of age, and included smokers, vapers, and asthmatics. Ethical consent for the trial was granted by the Human Ethics Committee at the University of Canterbury (Ref: HEC 2020/14/LR), with a later amendment confirming approval to publish the de-identified dataset.
Time, pressure and flow (both raw ADC output and processed/scaled results in relevant units) information is included in the dataset alongside de-identified relevant demographic/medical information for each subject. A README.txt file is included to describe the dataset details and structure. Recordings were 60 seconds in normal (resting) breathing, 50 seconds in both short and medium short breathing, 120 seconds in medium long breathing and 180 seconds in long recordings. A 1.5 second delay occurred at the start of each recording and files were trimmed in processing to include full breaths and remove any recording errors at the start or end of files.
This data has been transferred to CSV files. Processed Files are included with relevant units. Processed Files contain Time [s], Pressure at Venturi 1 [cmH20], Pressure at Venturi 2 [cmH20], Flow at Venturi 1 [L/s], and Flow at Venturi 2 [L/s] as column vectors from A to E respectively. Row 1 contains titles and units for the column values.
RAW Data files are also included with Time [s], Pressure at Venturi 1 [ADC], Inspiratory (positive) Flow at Venturi 1 [ADC], Expiratory (negative) Flow at Venturi 1 [ADC], Pressure at Venturi 2 [ADC], Inspiratory (positive) Flow at Venturi 2 [ADC], and Expiratory (negative) Flow at Venturi 2 [ADC] as column vectors from A to G respectively. Row 1 contains titles and units for the column values.
Usage Notes
This data could be used to develop or validate models of pulmonary mechanics and/or to develop methods to identify patient-specific parameters which cannot be measured non-invasively. These models and values, particularly if available breath-to-breath in real-time, could assist clinicians in the prescription or optimisation of CPAP therapy, including optimising PEEP settings. Establishing a method of extrapolating patient breathing effort from this data could also help in the prescription of ventilation therapy. It could provide another mode of feedback to clinicians on the efficacy of the CPAP therapy at given PEEP settings.
Release Notes
Addition of Figures 1-3 outlining the data collection method
Ethics
Ethical consent for the trial was granted on 16 JULY 2020 by the Human Ethics Committee at the University of Canterbury (Ref: HEC 2020/14/LR). An amendment on 19 MARCH 2021 confirmed the ability to publish the de-identified dataset.
Acknowledgements
This work was supported by the NZ Tertiary Education Commission (TEC) fund MedTech CoRE (Centre of Research Excellence; #3705718) and the NZ National Science Challenge 7, Science for Technology and Innovation (2019-S3-CRS).
Conflicts of Interest
The authors have no competing interests to declare.
References
- Sensirion. Datasheet SDP8xx-Analog. 2018.
- NXP. Integrated Silicon Pressure Sensor On-Chip Signal Conditioned, Temperature Compensated and Calibrated. 2008.
- Popat B, Jones AT. Invasive and non-invasive mechanical ventilation. Medicine. 2012;40(6):298-304.
- Burns KEA, Adhikari NKJ, Keenan SP, Meade M. Use of non-invasive ventilation to wean critically ill adults off invasive ventilation: meta-analysis and systematic review. BMJ. 2009;338:b1574.
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. European Respiratory Journal. 2005;26(5):948.
- Heinzer RC, Stanchina ML, Malhotra A, Fogel RB, Patel SR, Jordan AS, et al. Lung volume and continuous positive airway pressure requirements in obstructive sleep apnea. American journal of respiratory and critical care medicine. 2005;172(1):114-7.
- Howe SL, März M, Krüger-Ziolek S, Laufer B, Pretty C, Shaw GM, et al. Measuring lung mechanics of expiratory tidal breathing with non-invasive breath occlusion. BioMedical Engineering OnLine. 2020;19(1):32.
- Duncan AW, Oh TE, Hillman DR. PEEP and CPAP. Anaesthesia and intensive care. 1986;14(3):236-50.
- Rajdev K, Idiculla PS, Sharma S, Von Essen SG, Murphy PJ, Bista S. Recurrent Pneumothorax with CPAP Therapy for Obstructive Sleep Apnea. Case Reports in Pulmonology. 2020;2020:8898621.
- Yiallourou TI, Schmid Daners M, Kurtcuoglu V, Haba-Rubio J, Heinzer R, Fornari E, et al. Continuous positive airway pressure alters cranial blood flow and cerebrospinal fluid dynamics at the craniovertebral junction. Interdisciplinary Neurosurgery. 2015;2(3):152-9.
- Mercat A, Richard J-CM, Vielle B, Jaber S, Osman D, Diehl J-L, et al. Positive End-Expiratory Pressure Setting in Adults With Acute Lung Injury and Acute Respiratory Distress Syndrome: A Randomized Controlled Trial. JAMA. 2008;299(6):646-55.
- Oba Y, Thameem DM, Zaza T. High levels of PEEP may improve survival in acute respiratory distress syndrome: A meta-analysis. Respiratory Medicine. 2009;103(8):1174-81.
- FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Medical Ethics. 2017;18(1):19.
- Policy: CPAP Titration Protocol, (2019).
- Titration protocol reference guide. Koininklijke Philips NV: Philips Respironics; 2017.
- Goligher EC, Costa EL, Yarnell CJ, Brochard LJ, Stewart TE, Tomlinson G, et al. Effect of Lowering Tidal Volume on Mortality in ARDS Varies with Respiratory System Elastance. (ja).
- Bates JHT. Lung mechanics: an inverse modeling approach. Cambridge, UK;New York;: Cambridge University Press; 2009.
- Chiew YS, Chase JG, Shaw GM, Sundaresan A, Desaive T. Model-based PEEP optimisation in mechanical ventilation. BioMedical Engineering OnLine. 2011;10(1):111.
- Chiew YS, Pretty C, Docherty PD, Lambermont B, Shaw GM, Desaive T, et al. Time-varying respiratory system elastance: a physiological model for patients who are spontaneously breathing. PLoS One. 2015;10(1):e0114847-e.
- Morton SE, Knopp JL, Chase JG, Docherty P, Howe SL, Möller K, et al. Optimising mechanical ventilation through model-based methods and automation. Annual Reviews in Control. 2019;48:369-82.
- Chase JG, Preiser J-C, Dickson JL, Pironet A, Chiew YS, Pretty CG, et al. Next-generation, personalised, model-based critical care medicine: a state-of-the art review of in silico virtual patient models, methods, and cohorts, and how to validation them. BioMedical Engineering OnLine. 2018;17(1):24.
- Rees SE. The Intelligent Ventilator (INVENT) project: the role of mathematical models in translating physiological knowledge into clinical practice. Computer methods and programs in biomedicine. 2011;104 Suppl 1:S1-29.
- Rees SE, Allerød C, Murley D, Zhao Y, Smith BW, Kjærgaard S, et al. Using physiological models and decision theory for selecting appropriate ventilator settings. 2006;20(6):421-9.
- Redmond DP, Chiew YS, Major V, Chase JG. Evaluation of model-based methods in estimating respiratory mechanics in the presence of variable patient effort. Computer methods and programs in biomedicine. 2019;171:67-79.
- Chiew YS, Tan CP, Chase JG, Chiew YW, Desaive T, Ralib AM, et al. Assessing mechanical ventilation asynchrony through iterative airway pressure reconstruction. 2018;157:217-24.
- Kannangara DO, Newberry F, Howe S, Major V, Redmond D, Szlavecs A, et al. Estimating the true respiratory mechanics during asynchronous pressure controlled ventilation. 2016;30:70-8.
- Szlavecz A, Chiew YS, Redmond D, Beatson A, Glassenbury D, Corbett S, et al. The Clinical Utilisation of Respiratory Elastance Software (CURE Soft): a bedside software for real-time respiratory mechanics monitoring and mechanical ventilation management. Biomed Eng Online. 2014;13:140.
Access
Access Policy:
Anyone can access the files, as long as they conform to the terms of the specified license.
License (for files):
Creative Commons Attribution-ShareAlike 4.0 International Public License
Discovery
DOI (version 1.0.1):
https://doi.org/10.13026/xfae-vv63
DOI (latest version):
https://doi.org/10.13026/33rx-gh20
Topics:
peep
cpap
respiratory mechanics
pulmonary mechanics
respiratory modelling
biomedical engineering
Corresponding Author
Files
Total uncompressed size: 233.6 MB.
Access the files
- Download the ZIP file (89.4 MB)
-
Download the files using your terminal:
wget -r -N -c -np https://physionet.org/files/cpap-data-canterbury/1.0.1/
-
Download the files using AWS command line tools:
aws s3 sync s3://physionet-open/cpap-data-canterbury/1.0.1/ DESTINATION
| Name | Size | Modified |
|---|---|---|
| Processed_CSV_Data_Files | ||
| RAW_CSV_Data_Files | ||
| Figure1.png (download) | 9.3 KB | 2022-03-08 |
| Figure2.png (download) | 425.6 KB | 2022-03-08 |
| Figure3.png (download) | 34.3 KB | 2022-03-08 |
| LICENSE.txt (download) | 16.0 KB | 2022-03-24 |
| README.txt (download) | 1.6 KB | 2021-03-25 |
| SHA256SUMS.txt (download) | 78.6 KB | 2022-03-24 |
| SubjectDemographicData.csv (download) | 1.7 KB | 2021-05-01 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}